


One more essay on the Polyconflict before I shift back to the Planetarity Syllabus. I have several essays queued up, but am holding them back while I get these depressing thoughts out of my head.
A couple of days ago, I wrote about the impending Helium Shock due to the Gulf war. But Helium isn’t the only commodity under threat. It’s not even the only medically relevant commodity under threat. Surprise, surprise: the pharmaceutical industry is deeply dependent on the fossil fuel industry, and not just as an energy source: petrochemicals such as benzene and ethylene are the building blocks of modern drugs. Pharmaceuticals are petrochemicals!
In the two previous essays, I argued that polyconflicts cannot be managed from a control room. They are structural, open-ended scrambles for survival that must be traced node by node, commodity by commodity. We looked at how a drone strike in the Persian Gulf dictates the cost of a neurological MRI in Bihar by choking the global supply of helium. We saw how escaping one geopolitical trap frequently means wading into another.
The pharma industry is no different - the path to understanding the polyconflict is non-linear. I am going to illustrate that nonlinearity with a disease and a drug of great importance to Indians: diabetes and metformin respectively, where the metabology of the conflict is literally about human metabolism.
1. Diabetes
If you’re Indian, you almost certainly have a close family member who has diabetes, probably many such. According to the 2023 ICMR-INDIAB study, over 101 million Indians are currently living with diabetes, with an additional 136 million lingering in a state of pre-diabetes. We currently account for roughly one-quarter of the global diabetic burden.
Why are we so uniquely prone to diabetes?
It comes down to a metabolic profile known in the medical literature as the ‘Thin-Fat’ Indian phenotype. For epigenetic reasons due to nutritional stress and agrarian scarcity due to colonial era famines, Indians possess a lower metabolic capacity; we have smaller internal organs, particularly the pancreas and liver, and significantly less skeletal muscle mass. We are built to survive starvation, not abundance.
But we now live in an environment of unprecedented metabolic load. An Indian with a seemingly normal Body Mass Index (BMI) of 22 often carries the same hidden metabolic risk as a Caucasian with a BMI of 30. We are genetically predisposed to store our fat viscerally, packed around our internal organs and deep within our abdomens, rather than safely under the skin. This visceral fat is highly inflammatory. It triggers systemic insulin resistance and leads to premature beta-cell failure in the pancreas.
Unfortunately, nature and nurture have conspired to make the situation worse. Our biological vulnerability is exacerbated by the carb-heavy nature of our diet. Rice and wheat are the anchors of the Indian plate and palate. In the 1960’s, the threat of starvation - though there are serious doubts as to its accuracy - led to the Green Revolution and the massive expansion of monocultured grains in our diet.
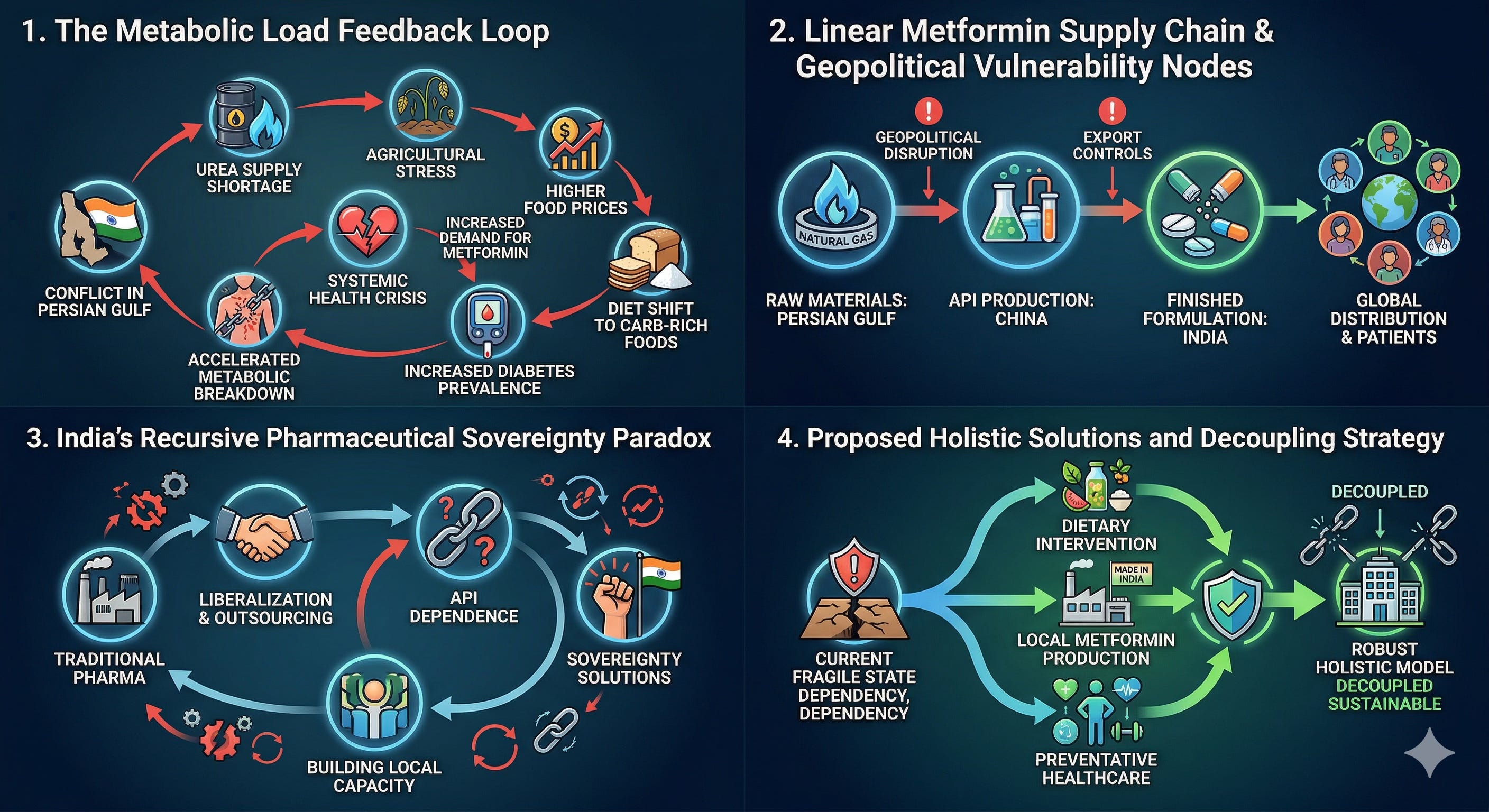
The cheap rice and wheat that sustains Indians are only made possible by the application of urea, a highly concentrated nitrogen fertilizer. India is dependent on the Persian Gulf for its urea. Over 45% of our urea imports come from Oman alone, with Qatar and Saudi Arabia providing much of the rest. With the Strait of Hormuz acting as a highly militarized choke point in the current Gulf War, the supply of urea is threatened. A urea shortage means drops in crop yields for the upcoming Kharif season.
Lower crop yields ➡️ inflation in agricultural staples.
When food inflation hits, you would be surprised to know that the pauper does not pivot to eating expensive lean proteins, imported quinoa, and fresh, organic vegetables. Instead, they default to the cheapest, most heavily processed, high-glycemic carbohydrates available on the market. Strange isn’t it? They eat more refined flour, more sugar, and more cheap starch because those are more affordable. IMHO, the war in the Gulf will lead to a more diabetogenic diet for a lot of people.
Just when our access to insulin regulating drugs like Metformin is about to decrease.
2. Metformin
If you are one of the hundred million Indians with diabetes, Metformin is likely keeping you alive. But what actually is Metformin? While its ancient origins trace back to the medicinal use of the French Lilac plant (Galega officinalis) in medieval Europe, modern Metformin is effectively solidified natural gas.
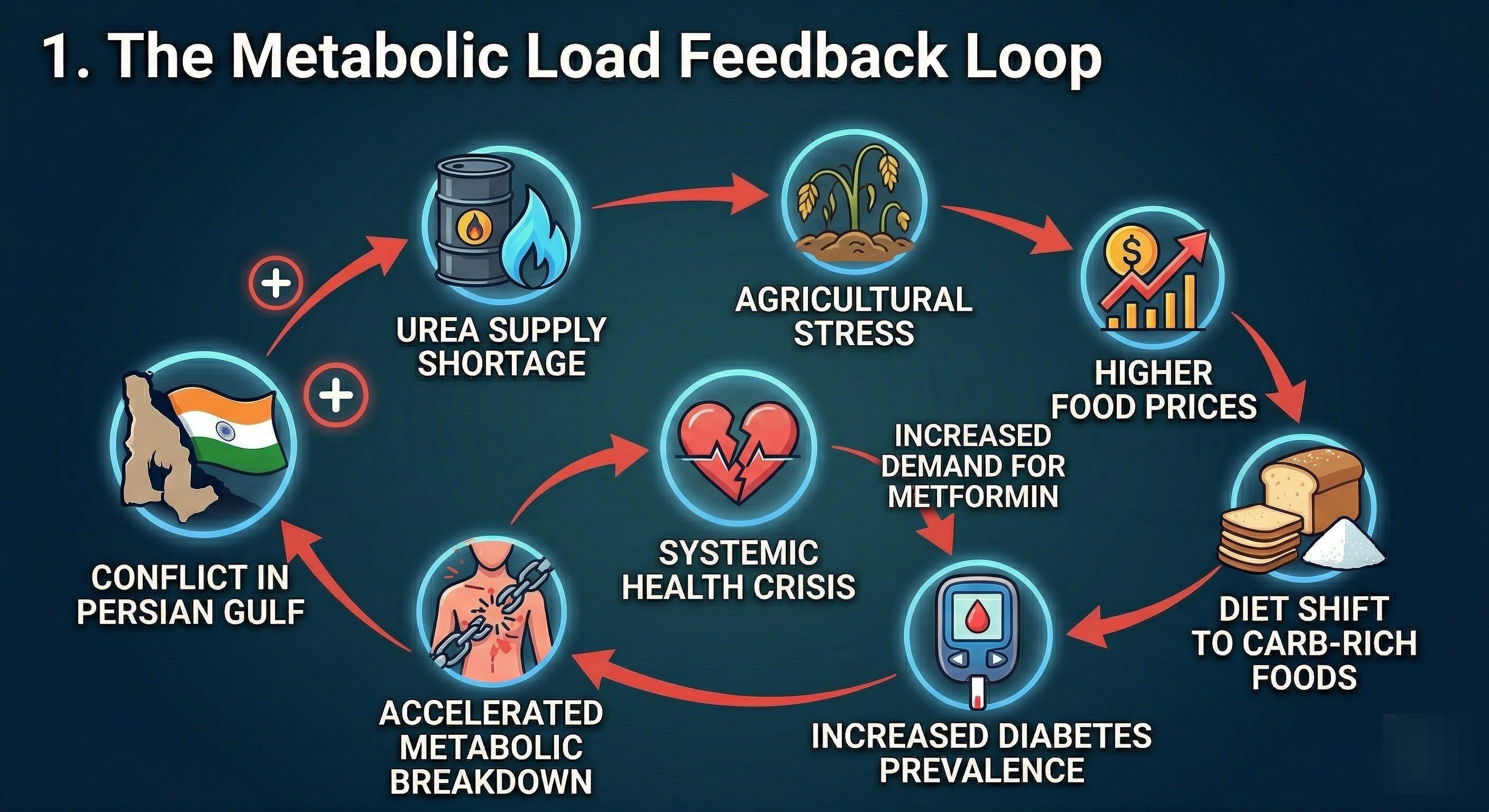
The industrial synthesis of Metformin relies on two chemical building blocks: Dimethylamine and Dicyandiamide. To manufacture Dimethylamine, a chemical plant requires enormous quantities of methanol and ammonia. To get methanol and ammonia, you need massive, continuous flows of methane (natural gas). To synthesize Dicyandiamide, you need nitrogen-rich feedstocks processed in energy-intensive, high-heat environments.
Therefore, the Metformin manufacturing cycle starts with the Persian Gulf. The industrial cathedrals of Qatar’s Ras Laffan complex and Saudi Arabia’s Jubail industrial city are the world’s sources for the methane and ammonia that go into Metformin. The former was lit on fire by Iranian missiles last week and the second has been threatened many times.
The threat to the Metformin supply chain is terrifying because of the drug’s indispensability. Globally, it is the undisputed first-line oral therapy for Type 2 diabetes. It works by activating the AMPK enzyme, essentially tricking the liver into halting its overproduction of glucose while making the body’s muscle tissues more sensitive to whatever insulin remains. It is cheap to produce, highly effective at lowering blood sugar, and unlike older drugs, carries a very low risk of inducing fatal hypoglycemia.
In India, Metformin is even more important. The ICMR guidelines position Metformin as the foundational treatment for almost all newly diagnosed patients. Because Indians experience beta-cell failure and crippling insulin resistance so much earlier in life - often diagnosed in their late 20s or 30s rather than their 60s - Metformin is prescribed aggressively and preemptively, even to lean, young patients who do not fit the Western profile of a diabetic.
Furthermore, the Indian pharmaceutical market is driven by Fixed-Dose Combinations (FDCs). In this model, Metformin is chemically combined with other drugs, like Glimepiride or Teneligliptin, into a single, high-density tablet to reduce the pill burden (the more pills you are asked to swallow, the less likely you’re going to take them all) for patients and ensure compliance.
In short: Metformin is the bedrock of India’s public health response to a crisis affecting 101 million citizens with another 136 million waiting in the wings. If the supply of Metformin is compromised, the edifice of Indian diabetes management is on shaky grounds, for there is no viable, scalable, equally affordable substitute. We cannot simply switch to $1000-a-month GLP-1 receptor agonists (like Ozempic) or afford complex, refrigerated insulin regimens. It is Metformin or nothing.
PS: Even more irony - the patent for Semaglutide (Ozempic and Wegovy) expired recently, and tons of Indian firms want to manufacture generic versions of these drugs, but for that to happen, Indian pharma needs petrochemicals from Qatar and KSA.
4. Upstream of Metformin - the China factor
If the Gulf provides the raw energy and base molecules, how does the pill actually get made? The answer isn’t flattering to India during a polyconflict.
TLDR; we saw in the first essay on this polyconflict that India has to walk the tightrope between the Gulf and China for its energy needs. Turns out, we have to play the same game for Metformin too.
The production of Metformin is split between China and India, with China acting as the upstream brick-maker, while India acts as the downstream house-builder. China currently dominates the global production of Active Pharmaceutical Ingredients (APIs) - the actual, synthesized medicinal chemicals that do the work in the body. As of 2024, China accounted for roughly 45% of all new global API filings. Massive, heavily subsidized Chinese chemical mega-factories in provinces like Shandong synthesize the Dimethylamine and Dicyandiamide into pure, bulk Metformin API.
India then imports these Chinese APIs by the megaton. In vast formulation plants in Hyderabad, Ahmedabad, and Mumbai, Indian companies press this Chinese powder into tablets, package them into aluminum blister packs, and ship them around the world. As of recent data, India relies on China for 70% to 80% of its total API and bulk drug imports.
Not to belabor the analogy too much, but this is the same model through which fentanyl enters the US: the Chinese make the precursor chemicals, ship them to Mexico where the cartels assemble fent and ship it to their markets in the US and and Europe.
If the Gulf War creates a severe energy shock, it hits China’s chemical factories first. China, prioritizing its own domestic stability and the health of its own massive population, can easily and instantly weaponize export controls. In a time of molecular scarcity, Beijing can restrict the export of Metformin API or the critical, energy-intensive solvents required to synthesize it. Indian generic manufacturers will be starved of their core ingredients, and will find their assembly lines paralyzed.
Why aren’t we making our own APIs? It turns out we used to, but....
5. How India Lost Its Pharmaceutical Sovereignty
It was not always this way. To understand how India fell into this disastrous double-bind, we must look at the history of our pharmaceutical industry, which tracks perfectly with the rise of neoliberal managerialism.
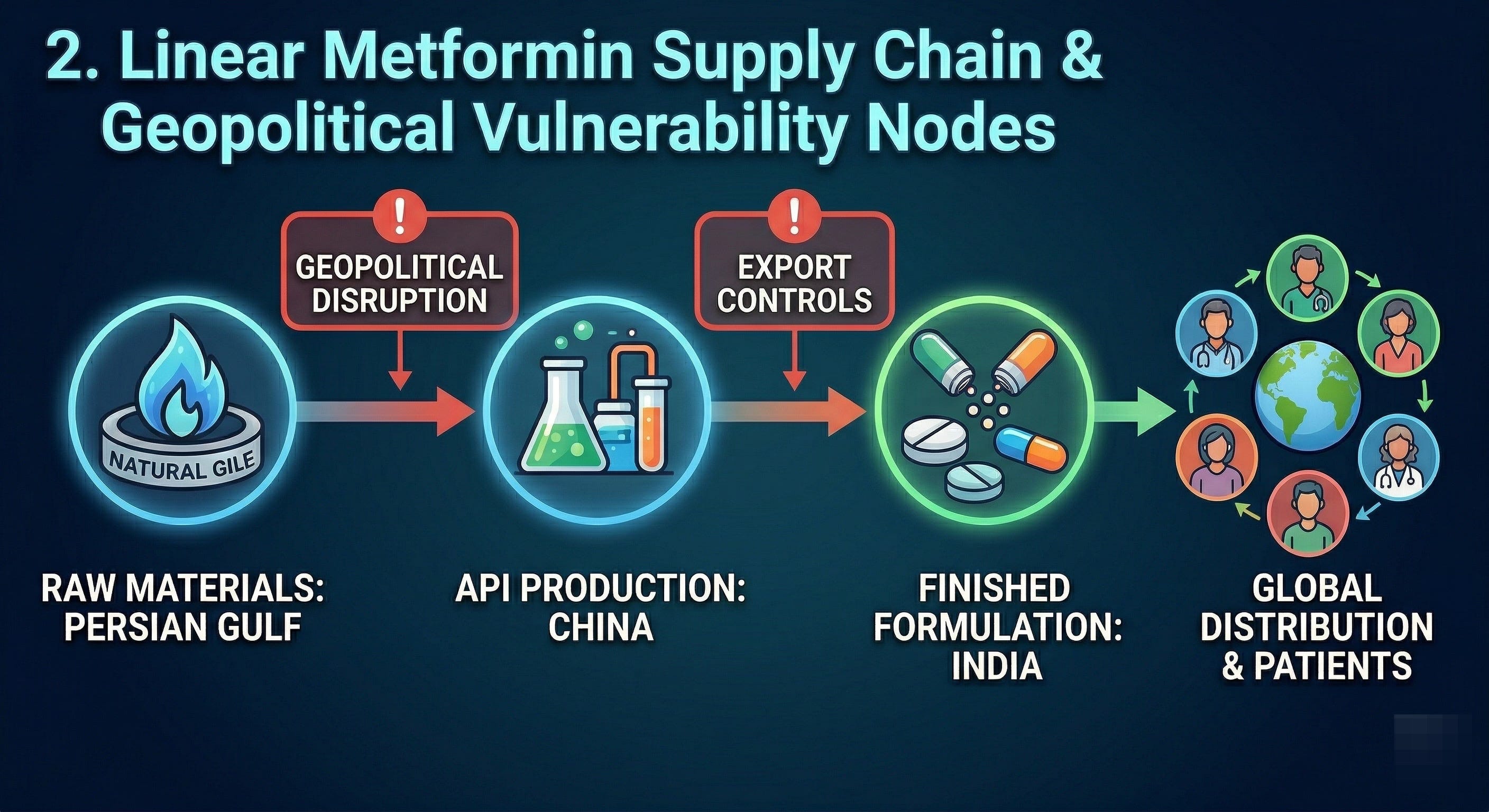
Following the Patents Act of 1970, which recognized process patents but not product patents, India built an independent, vertically integrated pharmaceutical sector. In the 1970s and 80s, Indian scientists reverse-engineered global blockbuster drugs and successfully manufactured the APIs domestically. We owned the chemistry. In 1991, Chinese ingredients made up less than 1% of India’s bulk drug imports.
But in the 1990s and 2000s, after liberalization, globalized capitalism took hold. Indian pharma CEOs realized that high profit margins lay in marketing the finished formulations to Western markets, not in the dirty, highly regulated, energy-intensive, low-margin business of chemical synthesis and fermentation. Simultaneously, China made a strategic state decision to capture the base of the global supply chain, building massive chemical mega-parks powered by cheap coal and heavily subsidized grids.

Makes sense from an individual pharma company’s POV: outsourcing API production to China was the rational choice. And so, India voluntarily hollowed out its own chemical foundation. We dismantled our fermentation plants and allowed our chemical synthesis capacity to wither because it was cheaper to buy the molecules from Shandong.
Today, as the Indian government scrambles to launch Production Linked Incentive (PLI) schemes to bring API manufacturing back to Indian soil, we face a brutal situation. To rebuild these energy-intensive API factories, India needs cheap, reliable power, stable grids, and raw petrochemical feedstocks. Where does that energy come from? The Persian Gulf or Chinese Solar manufacturers. The very attempt to escape our pharmaceutical dependence on China drives us deeper into our energy dependence on the Middle East and China.
A true polyconflict if there was one. There is no escape hatch, only a shifting of vulnerabilities from one sector to another.
6. Not Just India: The Generic Squeeze
India supplies roughly 40% to 50% of all the generic drugs consumed in the United States and the United Kingdom. If Chinese export curbs and Gulf energy shocks squeeze the Indian manufacturer in Hyderabad, the downstream effect hits the pharmacy shelf in London, Detroit, and Boston within weeks. The rationing hierarchy we saw with Helium - where hospitals compete for scarce resources - will replicate itself in pharmaceuticals.
The American and European working classes - already burdened by decaying, hyper-financialized healthcare systems - could be plunged into further medical debt just to afford basic metabolic maintenance. The pauper in Darbhanga and the pauper in Detroit are tethered to the same fragile supply chain.
7. The Perfect Storm: Inflation, Diet, and Disease
Let us return to India, where various macro-level shocks caused by the Gulf War converge into a perfect storm.
On one front, the cost of Metformin and other essential diabetes treatments could rise as API supply chains fracture, energy costs spike, and transportation insurance premiums surge. On another front, food inflation driven by fertilizer (urea) shortages will make healthy, protein-rich diets economically impossible for the majority of the population.
Imagine the daily reality of the tenant farmer in Bihar or the gig worker in Bengaluru: their diet is forced to become more carb-heavy, more ultra-processed, and more diabetogenic precisely at the historical moment when the medication required to manage the physiological fallout of that diet becomes scarce and expensive. We are looking at a negative spiral of human health and economic agency.
There are no quick answers to this polyconflict, but we can take steps to address the situation in the short as well as long term.
8. Interconnected Pathways
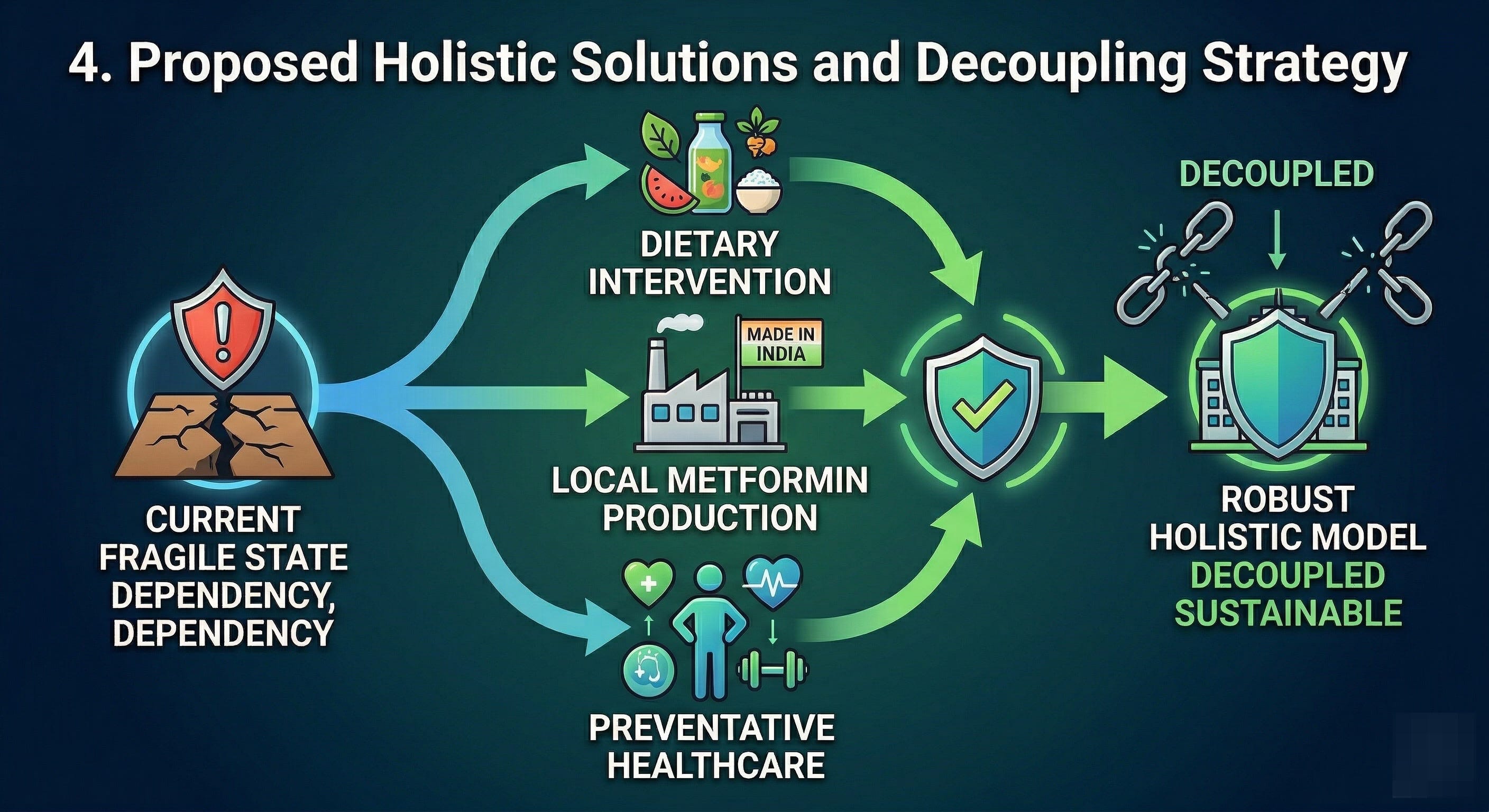
Because the threats to our biology and our economy are deeply interconnected, our solutions must be equally holistic. We simply address the pharmaceutical crisis without simultaneously addressing the agricultural crisis. I am well aware that I am out of my depth in most of these topics and my suggestions could well be laughable - but it’s better to put my views out there and invite rebuttal than to stay silent.
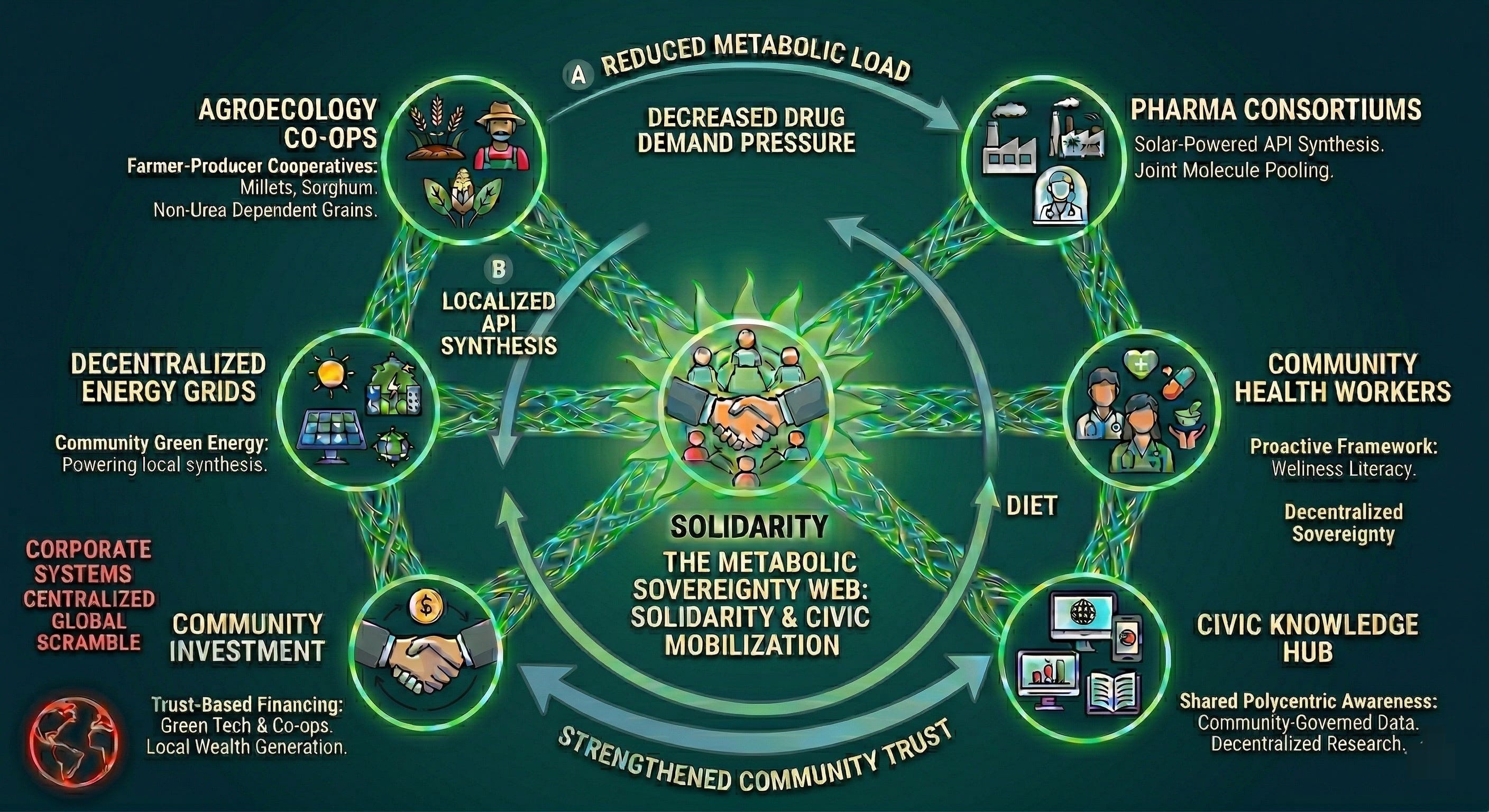
Food: We must aggressively pivot our agricultural systems away from fossil-fuel dependency. This is no longer just an environmental goal; it is a metabolic imperative. This means a structural shift toward agroecology and the large-scale cultivation of indigenous, climate-resilient grains like millets and sorghum, which require a mere fraction of the imported urea that paddy demands. A shift in agriculture forces a shift in diet - moving from refined, cheap carbs to local, protein-rich, complex carbohydrates that respect and nourish the Indian phenotype rather than poisoning it.
Pharma: The pharmaceutical industry must be insulated from foreign API supply shocks. This cannot simply mean building dirty, coal-fired plants in Maharashtra to mimic Shangdong. It requires pioneering localized API synthesis powered by decentralized green energy grids. We must treat the production of essential, life-saving medicines as critical, non-negotiable sovereign infrastructure, not just a high-margin export business.
Healthcare: We must fundamentally redefine healthcare from a reactive system of disease management via global drug regimes to a proactive, holistic framework of wellness, which has roots in local consumption patterns, community health literacy, preventive nutrition, and equitable access to localized medical facilities.
9. Commodity by Commodity: The Necessity of Solidarity
There is no master switch to turn off a polyconflict. Machiavelli’s grim insight remains entirely true for our era: systemic conflict is structural, and the prince who waits for stability before acting will wait forever.
These challenges must be resolved commodity by commodity, molecule by molecule.
We desperately need state intervention to heavily subsidize local food systems, fund indigenous pharmaceutical technology, and protect local manufacturing from global dumping. But the state alone is too slow, too cumbersome, and too easily captured by capital.
Therefore, we also need a massive, unprecedented mobilization of civic networks too. Solidarity is the only rational and moral response to a world where the conflicts are simply too large, too complex, and too planetary for any individual to survive alone. We must urgently weave localized, cooperative safety nets such as farmer-producer cooperatives sharing agroecological knowledge. We also need pharmaceutical consortiums pooling API resources and intellectual property, and community health workers prioritizing wellness over corporate margins.
What else?
PS: I hope you are getting a sense of my approach to system analysis: the earthworm’s way, so to speak.
Instead of talking about economic or political crises from a purely macro lens, it’s better to narrow down to one issue or commodity and trace its interconnections - they are far more likely to throw surprises than the view from up above, as I learned by tracing those connections for Helium as well as Metformin.
I am confident you can do this type of trace-analysis in every sector.
Really brought it home with this one!! All the more reason for public health awareness and action based initiatives, guerrilla gardening of vegetables in community spaces. I'm starting to feel like when we left Gandhi behind we dug our own graves... We need self sufficiency at the neighbourhood level onwards to survive all that is coming our way.
As a diabetic relying on metformin daily, this is eye opening. Also appreciating how you approach things from a zoomed-in lens to see its interconnections.